




Abdominal Wall Reconstruction Surgery By Dr. Saurabh Kalia
Abdominal wall reconstruction surgery is the practice of taking a dysfunctional abdominal wall due to hernia disease and putting it back together using advanced surgical techniques. Abdominal wall reconstruction is reserved for large, more complex, or recurrent hernias.
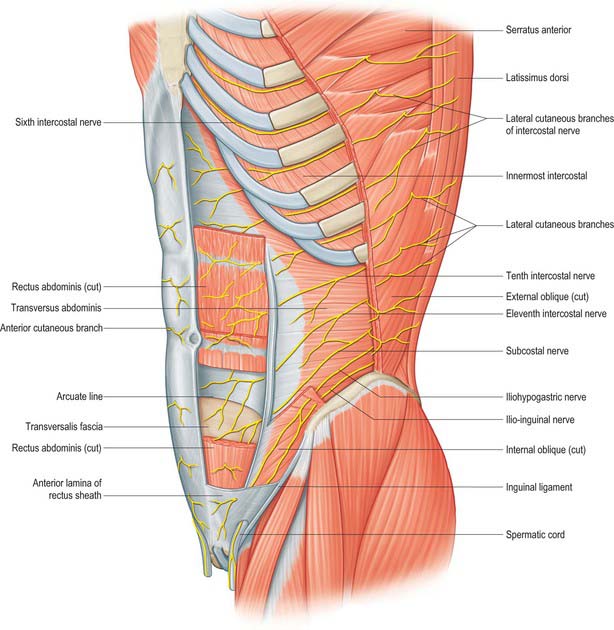
The Abdominal Wall
The abdominal wall is one of the most complex anatomic structures in the human body. Each of the muscles interconnect with each other, and the function of the abdominal wall is dynamic and complex in nature.
The major muscles that we attempt to reconstruct are the:
- Rectus abdominis
- External oblique
- Internal oblique
- Transversus abdominis.
Due to the complexity of certain hernias, repairing them with simple sutures may not be enough. In certain cases, a reconstructive procedure called a component separation may be necessary. This involves making incisions in 1 of the 3 oblique muscles in order to close the hernia. Long-term studies have shown that this technique does not interfere with the function of your abdominal wall and may be the only way to close large defects.
Abdominal wall surgery may be performed using:
- An open technique with traditional incisions
- Laparoscopic technique using small incisions
- Robotic technique using small incisions
Small incisions are generally preferred, but there are often reasons that make an open approach better, such as the difficulty in closing incisions, or the need to remove redundant tissue or skin.
There are several surgical procedures that fall under the category of reconstruction. These include:
Retro-Rectus Rives Stoppa Repair
This involves cutting the connective tissue, or fascia, around the ab muscles to flatten them and bring them together.
This technique attempts to re-approximate your rectus abdominis muscles and repair the hernia at the same time. Mesh is placed behind your ab muscles.
Anterior Component Separation
This surgery involves making a cut in one of your oblique muscles (the external oblique) so that your hernia can be repaired without tension. The incision into that muscle has no meaningful affect on your future core function after you heal.
With this approach, mesh is placed between the skin of the abdominal wall and the ab muscles.

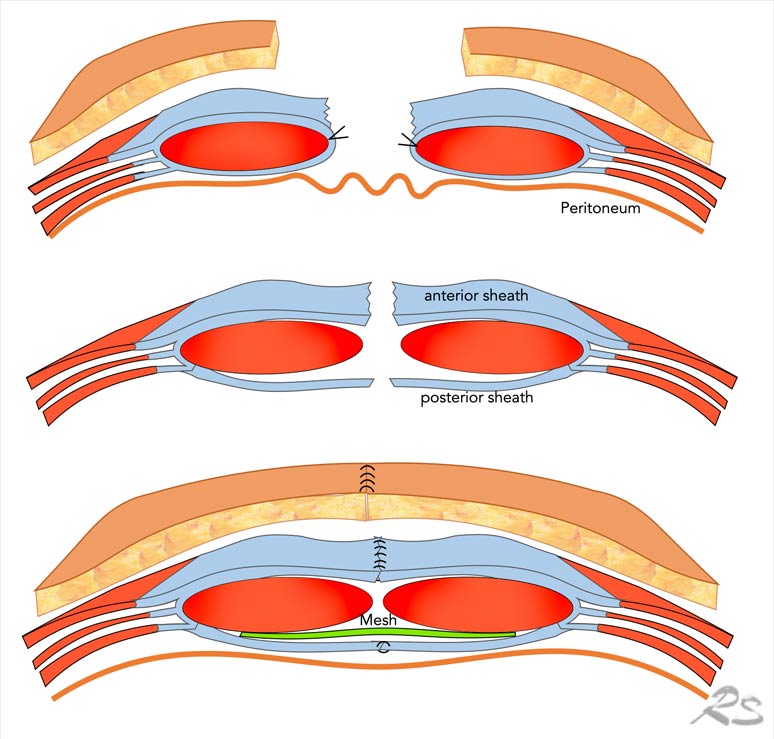
Posterior component separation, or Transversus Abdominis Release (TAR)
This involves cutting the transversus abdominis muscle, the innermost of our oblique muscles.
This surgery is more complex than the Rives-Stoppa techniques, in that to assist with closing large hernia defects, a cut is made in one of your oblique muscles (the transversus abdominis) so that your hernia can be repaired without tension. This incision into that muscle has no meaningful affect on your future core function after you heal.
Mesh is placed between the lining of the abdominal wall and the ab muscles.
Mesh and Abdominal Wall Reconstruction
In abdominal wall surgery, permanent or semi-permanent mesh drastically reduces the risk of recurrence in the future, as it assists with scar tissue formation to form your “new” abdominal wall.
There is always a risk of synthetic or biologic mesh complications, such as infection, erosion, or chronic pain. These risks can be reduced by placing the mesh in a space which has no contact with bowel and using techniques which do not expose any abdominal wall nerves. This provides a natural barrier between any intestine and the mesh.
What to expect from abdominal reconstruction surgery
Immediately after Surgery
You may have some mild upper abdominal or shoulder pain after surgery which can be normal since surgeons use carbon dioxide to fill your abdomen during surgery and this can get trapped. The gas is absorbed over the next 1-2 days but can be very uncomfortable in certain circumstances. Typically walking around and taking deep breaths can help absorb this air and reduce pain.
You may feel that your breathing is difficult. Again, this may be from pain, or the surgery, but if you feel this is getting worse then alert your doctor.
You will be given a small, handheld device called an incentive spirometer to help you take slow, deep breaths. These breathing exercises help your lungs recover from surgery. Use your incentive spirometer ten times every hour.
For pain control, we will attempt to use non opioid therapy, however in larger cases this may be impossible due to pain from large incisions.
We will also give you medicine to help with blood clots (heparin or lovenox injection), medicine for nausea, as well as forms of medicine you were taking at home
Complications of abdominal reconstruction are rare, and include but are not limited to:
- Pneumonia or telectasis (lung collapse)
- Wound infection, wound dehiscence (falling apart), abscess
- Urinary tract infection, inability to urinate
- Bowel damage
- Blood clots
- Chronic pain
- Need for additional surgery
Tips for a successful recovery from abdominal wall surgery
- Diet after abdominal wall surgery
- Stick to a light, soft diet for the first 2-3 days after surgery.
- Incision Care
- Please keep your incisions clean and dry. Replace dressings if soaked
Notify your surgeon if there is discoloration, redness, swelling, pain, or drainage from your incisions.
Abdominal Binder
For some cases you may have an abdominal binder placed. Please wear the binder while awake for 4 weeks total if given one.
These binders are typically machine washable, and additional ones can be purchased from pharmacies or online.
Drain Care
If you have a drain that you take home, remember it is sutured to your skin. You can prevent it from hanging or pulling by taping the tubing to the outside of your abdominal binder.
Empty the drain 1 time daily and record the amount of fluid.
Activity
- Avoid lifting anything more than 10 kg for 4 weeks.
- It is ok to walk up the stairs with the proper assistance (if needed).
- Do not drive if taking narcotic pain medications or while in moderate pain.
- Be sure to take focused deep breaths to help prevent lung collapse or pneumonia.
- Move around the house at least once an hour to prevent blood clots.
- After 4 weeks you can slowly transition to your normal routine without restrictions. If you notice pain or discomfort, you may need an additional week or two.
Remember, your abdominal muscles are busy recovering. You may have some back pain as a result, especially if you had it prior. You can alternate ice and heat on your back.
Please do not strain or bear down too much to have a bowel movement. This can cause undue stress on your surgery sites. Take stool softeners
Make sure to move around at least once an hour while awake. Long walks are recommended, even if only inside your dwelling.
Robotic Surgery in Abdominal Wall Reconstruction
The status of robotic surgery in abdominal wall reconstruction procedures has been evolving over the past decade.
Abdominal wall reconstruction (AWR) is a complex surgical field that involves repairing defects or hernias in the abdominal wall, often arising from previous surgeries or other abdominal conditions.
Over the last 10 years, robotic surgery has gained recognition and acceptance in abdominal wall reconstruction procedures. The da Vinci Surgical System, a widely used robotic platform, has been employed to enhance the precision and capabilities of surgeons in these intricate surgeries.
Advancements in robotic technology have allowed for improved manipulation of tissues, suturing, and reconstruction of the abdominal wall. The articulated robotic arms provide surgeons with increased dexterity, enabling them to navigate through challenging anatomical structures with greater ease. This enhanced precision is particularly valuable in AWR, where the complexity of the procedure demands meticulous attention to detail.
The minimally invasive nature of robotic surgery aligns well with the goals of AWR procedures. Small keyhole incisions allow for the insertion of robotic instruments, minimizing trauma to the abdominal wall. This approach has the potential to reduce postoperative pain, shorten hospital stays, and expedite patient recovery compared to traditional open techniques.
However, challenges persist, including the initial cost of acquiring and maintaining robotic systems, as well as the need for specialized training for surgeons. Despite these challenges, the advantages offered by robotic surgery in terms of improved visualization and precise tissue manipulation have contributed to its increased adoption in abdominal wall reconstruction.
As technology continues to advance, ongoing research and clinical studies are likely to further explore and refine the role of robotic surgery in abdominal wall reconstruction. Integration with artificial intelligence and the development of more sophisticated robotic platforms may contribute to expanding the applications of robotic-assisted techniques in this specific surgical domain. Unlock the benefits of Robotic Hernia Surgery in Jaipur with Dr. Saurabh Kalia, offering state-of-the-art procedures that prioritize patient well-being and recovery.
Also Read
